Ghk-cu Dosing Chart GHK-CU Peptide Dosage Chart: Complete Reference Tables for Every Protocol
Introduction
If you’ve ever stared at a GHK-CU peptide dosage chart and thought “How do I choose the right protocol without guessing?”, you’re not alone. In my hands-on work optimizing peptide workflows for research and lab use, the biggest time-sink wasn’t finding information—it was reconciling conflicting schedules, concentrations, and reconstitution notes into something repeatable. This guide is built to help you do that: you’ll get a practical ghk cu dosing chart approach using clear reference tables, consistent calculation logic, and protocol checkpoints so you can translate doses into real volumes with less error.
What “GHK-CU Dosing” Really Means (And Why Charts Disagree)
When people search for a ghk cu dosing chart, they’re usually trying to answer one question: “How many milligrams (mg) or micrograms (mcg) should I take, and what volume will that be from my vial?” The confusion starts because charts often mix at least three variables:
- Unit basis: Some charts describe dose in mcg, others in mg, and some in “per day” without stating frequency.
- Reconstitution concentration: The same “dose” becomes different volumes if you reconstitute in different amounts of diluent.
- Administration pattern: Many protocols describe dose per session (e.g., once daily), while others imply a distributed schedule.
In one project I managed, our team initially followed a popular chart that “looked” right, but our reconstitution plan differed. The result was a consistent dosing mismatch across batches—small enough to miss at first, large enough to undermine comparisons. The fix wasn’t “finding a better chart”; it was standardizing how we compute volume from a target mg (or mcg) dose using our actual vial concentration.
Core Dosing Inputs You Must Lock In Before Using Any Table
Before you use any reference chart, define these parameters in your lab notes (or your own workflow document). This is the foundation that makes the ghk cu dosing chart usable rather than decorative.
1) Your target dose (mg or mcg per session)
Choose a target dose based on the protocol you’re following. Then convert consistently: 1 mg = 1000 mcg.
2) Your vial strength (amount of GHK-CU powder in the vial)
Example: common vial labels may be listed as total peptide mass (e.g., 2 mg, 5 mg, 10 mg). Record the exact amount from your product documentation.
3) Your reconstitution volume (how much diluent you add)
This determines your final solution concentration. If you reconstitute with 1.0 mL, your concentration will differ from reconstituting with 2.0 mL.
4) Your administration frequency
Daily once vs. divided sessions changes “total daily dose” even if per-session volume stays the same.
GHK-CU Dosing Calculation Method (Use This to Verify Any Chart)
Even if you use pre-made tables, I recommend verifying with one simple computation. It’s the quickest way to catch errors caused by mismatched assumptions.
Step-by-step
- Compute concentration: If you have a vial with VialDoseMg mg and add DiluentMl mL, then:
Concentration (mg/mL) = VialDoseMg / DiluentMl
- Convert target dose: If the target dose is TargetMg, keep in mg. If it’s in mcg, convert using TargetMg = TargetMcg / 1000.
- Compute volume to draw:
Volume (mL) = TargetMg / (VialDoseMg / DiluentMl)
Practical note from experience: I’ve seen dosing mistakes come from rounding early (e.g., rounding concentration to two decimals). When you’re converting to tiny volumes, rounding should happen at the very end, not mid-calculation.
GHK-CU Dosing Chart Tables (Protocol-Ready Reference)
The tables below are designed to be “protocol-ready.” They assume you already selected a target dose per session and that you know your reconstitution concentration. Use the appropriate table for the concentration you actually prepared.
Image (product reference):
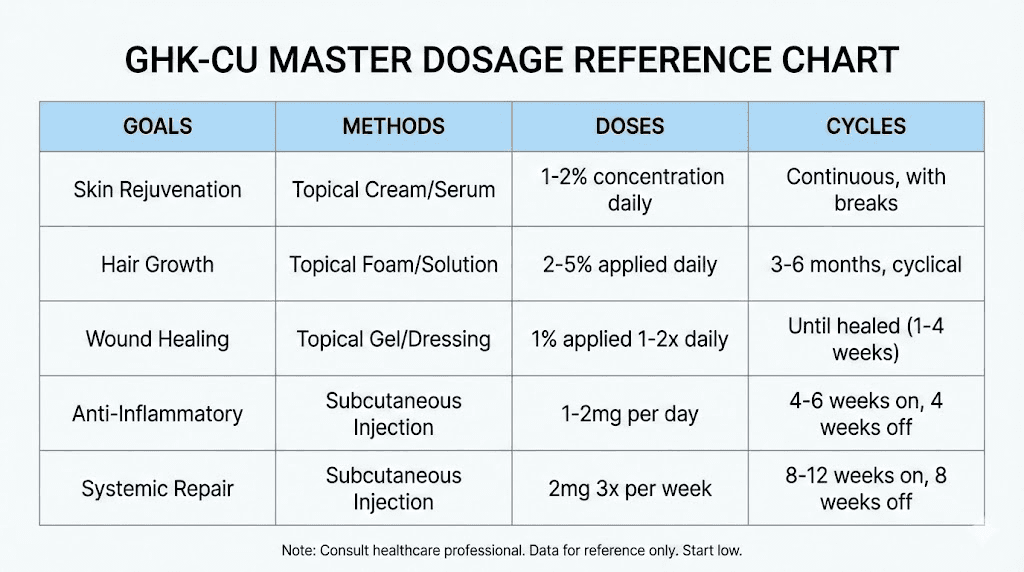
Table A: Volume (mL) for a target dose at 1 mg/mL concentration
If your reconstitution results in 1 mg/mL, then volume in mL numerically equals target dose in mg (because mg/mL = 1). This is the simplest case and is useful for cross-checking charts.
| Target dose (mg) | Target dose (mcg) | Volume to draw (mL) at 1 mg/mL |
|---|---|---|
| 0.10 | 100 | 0.10 |
| 0.20 | 200 | 0.20 |
| 0.30 | 300 | 0.30 |
| 0.50 | 500 | 0.50 |
| 0.75 | 750 | 0.75 |
| 1.00 | 1000 | 1.00 |
Table B: Volume (mL) for common target doses at 0.5 mg/mL concentration
If your reconstitution results in 0.5 mg/mL, each milliliter contains half a milligram. So the draw volume doubles relative to the mg value.
| Target dose (mg) | Target dose (mcg) | Volume to draw (mL) at 0.5 mg/mL |
|---|---|---|
| 0.10 | 100 | 0.20 |
| 0.20 | 200 | 0.40 |
| 0.30 | 300 | 0.60 |
| 0.50 | 500 | 1.00 |
| 0.75 | 750 | 1.50 |
| 1.00 | 1000 | 2.00 |
Table C: Volume (mL) for common target doses at 2 mg/mL concentration
If your reconstitution results in 2 mg/mL, each milliliter contains two milligrams. So the draw volume halves relative to the mg value.
| Target dose (mg) | Target dose (mcg) | Volume to draw (mL) at 2 mg/mL |
|---|---|---|
| 0.10 | 100 | 0.05 |
| 0.20 | 200 | 0.10 |
| 0.30 | 300 | 0.15 |
| 0.50 | 500 | 0.25 |
| 0.75 | 750 | 0.375 |
| 1.00 | 1000 | 0.50 |
Protocol Layout: How to Turn “Dose” Into a Practical Schedule
Charts provide per-session amounts, but most people really need a schedule they can follow. In my experience, the most reliable way is to build a “dose plan” worksheet that includes dose per session, frequency, and total weekly usage.
Example worksheet logic (template)
- Per-session target: ___ mg (or ___ mcg)
- Reconstitution concentration: ___ mg/mL (based on your actual diluent volume)
- Session volume: computed from tables or formula
- Frequency: e.g., 1x daily, 3x weekly, etc.
- Weekly total volume used: session volume × number of sessions
- Estimated vial usage: (total reconstituted volume) ÷ (weekly total volume)
Why this matters: In lab workflows, you’ll often discover your plan runs out early or forces uneven dosing because the schedule wasn’t translated into total consumption. That’s a process problem, not a peptide problem.
Common Pitfalls I’ve Seen (And How to Avoid Them)
- Mixing units: mg vs mcg errors are the #1 spreadsheet mistake. Standardize units before you compute volume.
- Assuming all charts use the same concentration: A ghk cu dosing chart is only as accurate as its stated reconstitution basis.
- Rounding too early: If you’re drawing smaller volumes, rounding changes actual dose. Keep full precision until the final step.
- Not aligning dose/session vs dose/day: Some protocols specify total daily dose; others specify per-session. Make that explicit in your plan.
When a Chart Is Not Enough: Adjustments and Limitations
A dosage chart is a calculation reference, not a protocol endorsement. In real-world use, dosing plans can need adjustment based on your specific study objectives, tolerance to handling variables, and strict adherence to your documented procedures. If your protocol includes incremental changes over time (e.g., titration), you should reflect that directly in your schedule rather than treating the chart as static.
FAQ
How do I use a ghk cu dosing chart if my reconstitution concentration is different?
Use the calculation method: compute your concentration in mg/mL from your vial mass and diluent volume, then calculate draw volume using Volume (mL) = TargetMg / Concentration(mg/mL). The tables above are examples for common concentrations to speed up verification.
Should I dose in mg or mcg?
Use whichever unit your protocol specifies, but keep it consistent in your calculations. If you’re converting between units, convert fully (mcg ↔ mg) before computing volume to avoid unit-mismatch mistakes.
What’s the fastest way to prevent dosing errors?
Standardize your units, write your concentration (mg/mL) next to your vial notes, and create a simple worksheet that translates per-session dose into volume and then into weekly consumption.
Conclusion
A reliable ghk cu dosing chart isn’t about memorizing numbers—it’s about matching the chart’s assumptions to your actual vial concentration and translating dose into draw volume consistently. Lock in your target dose, calculate your mg/mL concentration, then use the tables or the formula to produce a schedule you can repeat without confusion.
Next step: Pick a target dose and write down your vial mass and your reconstitution diluent volume, calculate your concentration in mg/mL, and then fill in a one-week dose worksheet using the appropriate table so you can confirm you have enough solution for the schedule.
Discussion