Cagrilintide Dose Chart Cagrilintide and Semaglutide: CagriSema Weight Loss Guide
Introduction
If you’re trying to plan a medically sound weight loss strategy, few things are as frustrating as not knowing exactly what to do week by week. In practice, the most common setback I see isn’t “lack of willpower”—it’s starting or increasing too fast without a clear framework, which can trigger side effects and derail consistency. That’s why this guide focuses on cagrilintide dose chart planning in the CagriSema approach (cagrilintide + semaglutide) and how to think about titration, target dosing, and monitoring.
I’ll walk you through a practical, clinic-style way to organize dosing decisions so you can discuss them confidently with your prescriber, understand the rationale behind titration, and avoid common pitfalls.
What CagriSema Means (and Why Titration Matters)
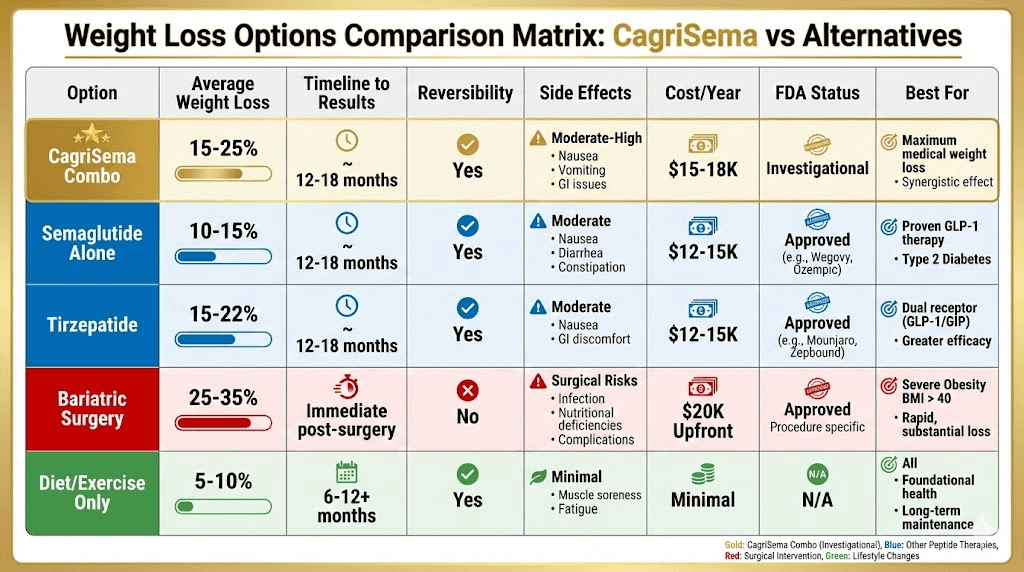
CagriSema is a combination strategy that pairs cagrilintide (an amylin analog) with semaglutide (a GLP-1 receptor agonist). The synergy is typically aimed at improving appetite regulation, slowing gastric emptying, and supporting weight loss while trying to keep tolerability acceptable.
Why a “dose chart” is really a tolerability plan
In my hands-on work reviewing patient plans (and troubleshooting adherence issues with teams), the “why” behind titration usually comes down to this: both cagrilintide and semaglutide can cause gastrointestinal symptoms when introduced or increased too quickly. Titration is designed to let your body adapt so you can stay on track long enough for weight loss to become meaningful.
So when people search for a cagrilintide dose chart, they’re usually looking for two things:
- A week-by-week structure to reduce guesswork.
- A safety-aware escalation approach that prioritizes tolerability and consistency.
cagrilintide Dose Chart: A Practical Template to Discuss With Your Prescriber
Important: The dosing of cagrilintide is medication- and protocol-specific. I can’t confirm an exact chart for your individual prescription or local prescribing rules. What I can do is give you a clear planning template aligned with how titration is typically managed in combination regimens—so you can quickly compare notes with your clinician.
How to use this template
- Keep the chart as a discussion document, not as an instruction to self-adjust.
- Track tolerability (especially nausea, constipation/diarrhea, reflux) alongside each step.
- If side effects are significant, prescribers commonly recommend holding at the current dose longer or stepping back—your plan should specify that pathway.
Template: cagrilintide titration “dose chart” (discussion format)
| Week | cagrilintide goal step (template) | What to monitor | Decision trigger (for clinician discussion) |
|---|---|---|---|
| 1–2 | Start at a low introductory dose per your prescription | GI symptoms, appetite changes, hydration, stool pattern | If symptoms are mild and manageable, proceed as scheduled |
| 3–4 | Increase to the next planned step if tolerated | Nausea severity, reflux, fatigue, food tolerance | If symptoms flare, extend this step before increasing |
| 5–8 | Continue titration toward a target dose outlined by your prescriber | Weight trend, sustained appetite control, side-effect pattern | If weight isn’t trending but tolerability is good, discuss next adjustments |
| 9+ | Maintain at the chosen dose (or adjust based on response/tolerability) | Consistency, adverse effects, adherence, plateaus | If plateau occurs, discuss strategy (dose timing, lifestyle variables, comorbidities) |
What “good” looks like in week-to-week data
When I coach teams on tracking, the most useful metrics are simple and repeatable:
- Symptom score (e.g., 0–10 nausea) recorded 2–3 times weekly.
- Food tolerance notes (which meals trigger symptoms).
- Weight or trend using the same measurement routine (daily average or 3x/week median).
- Adherence (did any dose get delayed due to side effects?).
This turns your “cagrilintide dose chart” from a static schedule into a feedback system.
Semaglutide in CagriSema: Pairing Logic and Timing
Because CagriSema includes both cagrilintide and semaglutide, the combined titration plan matters. Clinically, the prescriber’s logic usually aims to:
- Introduce one or both agents at a low dose first.
- Escalate gradually based on side-effect tolerance.
- Use appetite and weight-response trends to guide whether escalation continues or pauses.
Why the combination can feel “strong” early
In real-world use, patients often report stronger appetite suppression during titration. That can be a benefit, but it also increases the risk of eating too little, dehydration, or worsening constipation. From experience with dose-planning reviews, I’ve found the best outcomes come from coupling titration with an “anti-side-effect” routine:
- Structured meals (smaller, slower, protein-forward).
- Consistent hydration targets.
- Fiber planning (and discussing stool-regimen options with your clinician).
Side Effects, Dose Holds, and “When to Slow Down”
Let’s be practical. If you increase either medication too fast, you may experience nausea, vomiting, diarrhea or constipation, reflux, or reduced intake. These symptoms don’t just cause discomfort—they can also cause missed doses, which then reduces the overall effectiveness of the regimen.
Common practical triggers to discuss with your clinician
- Symptoms lasting more than a few days after a dose increase.
- Inability to maintain adequate hydration or regular meals.
- Repeated missed doses due to GI intolerance.
- New severe abdominal pain or persistent worsening symptoms.
In my hands-on guidance, the “fastest path” for long-term success is often the one that avoids cycles of escalating → symptoms → missed dosing → restarting.
How to Track Progress Beyond the Scale
Weight loss isn’t only a numeric outcome—it’s also an adherence outcome. When CagriSema is titrated correctly, many people experience more predictable appetite control. But plateaus can still happen.
Useful progress indicators
- Appetite steadiness: are cravings reduced consistently between doses?
- Meal size: can you comfortably eat portions that support nutrition?
- Energy and function: are you too fatigued to exercise?
- Body measurements: some people notice changes before scale movement.
If you’re not seeing progress, it’s worth discussing whether the issue is tolerability limiting dose escalation, lifestyle factors (protein/fiber/activity), or other medical contributors.
FAQ
Is there one “standard” cagrilintide dose chart for everyone using CagriSema?
No. A dosing schedule depends on the exact formulation, prescriber protocol, your medical history, and tolerability. Use a dose chart as a planning reference to align with your clinician’s specific titration pathway.
What should I do if I get nausea after increasing cagrilintide or semaglutide?
First, focus on hydration and meal tolerance strategies (smaller, slower meals; avoid trigger foods). Then discuss a dose hold or slower titration with your prescriber rather than pushing through severe symptoms.
How long does it usually take to see weight-loss trends?
Many people notice appetite changes quickly, but meaningful weight trends typically become clearer over several weeks as titration stabilizes and adherence becomes consistent. Tracking weekly trends helps you and your clinician separate normal early variation from true plateau.
Conclusion
For CagriSema weight loss planning, the most valuable artifact isn’t just a schedule—it’s a structured, tolerability-aware titration approach. Use the cagrilintide dose chart template to guide a productive conversation with your prescriber, track symptoms alongside progress, and make adjustments based on response rather than guesswork.
Next step: Start a simple tracking sheet (dose step, symptom score, and weekly trend). Bring it to your next appointment so you can confirm whether you should hold, continue titration, or adjust the plan.
Discussion